
Actualmente no hay pruebas lo suficientemente sensibles o específicas para confirmar el diagnóstico de PTI, por lo que sigue siendo de exclusión.1,2

Recomendaciones para el diagnóstico
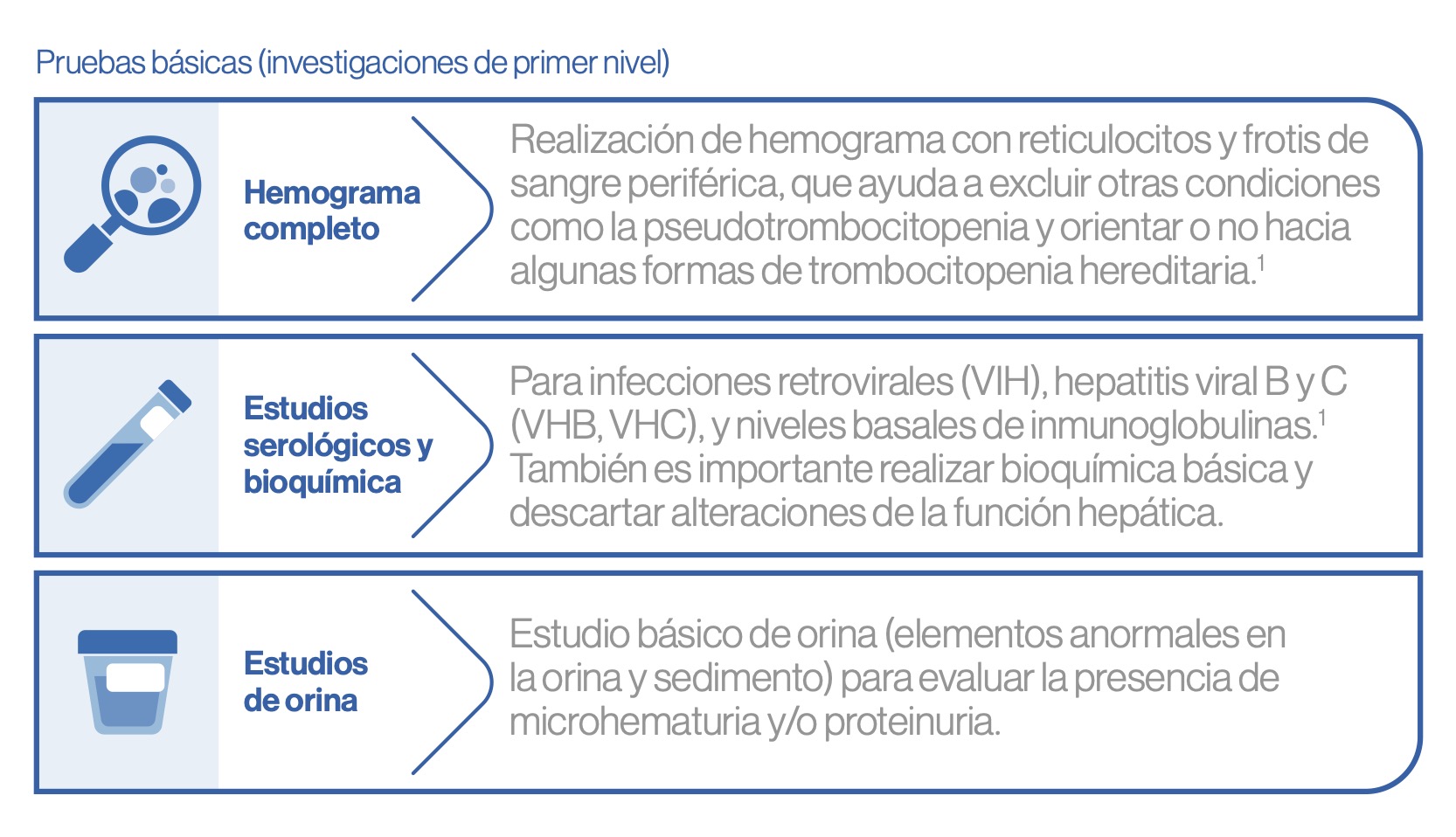
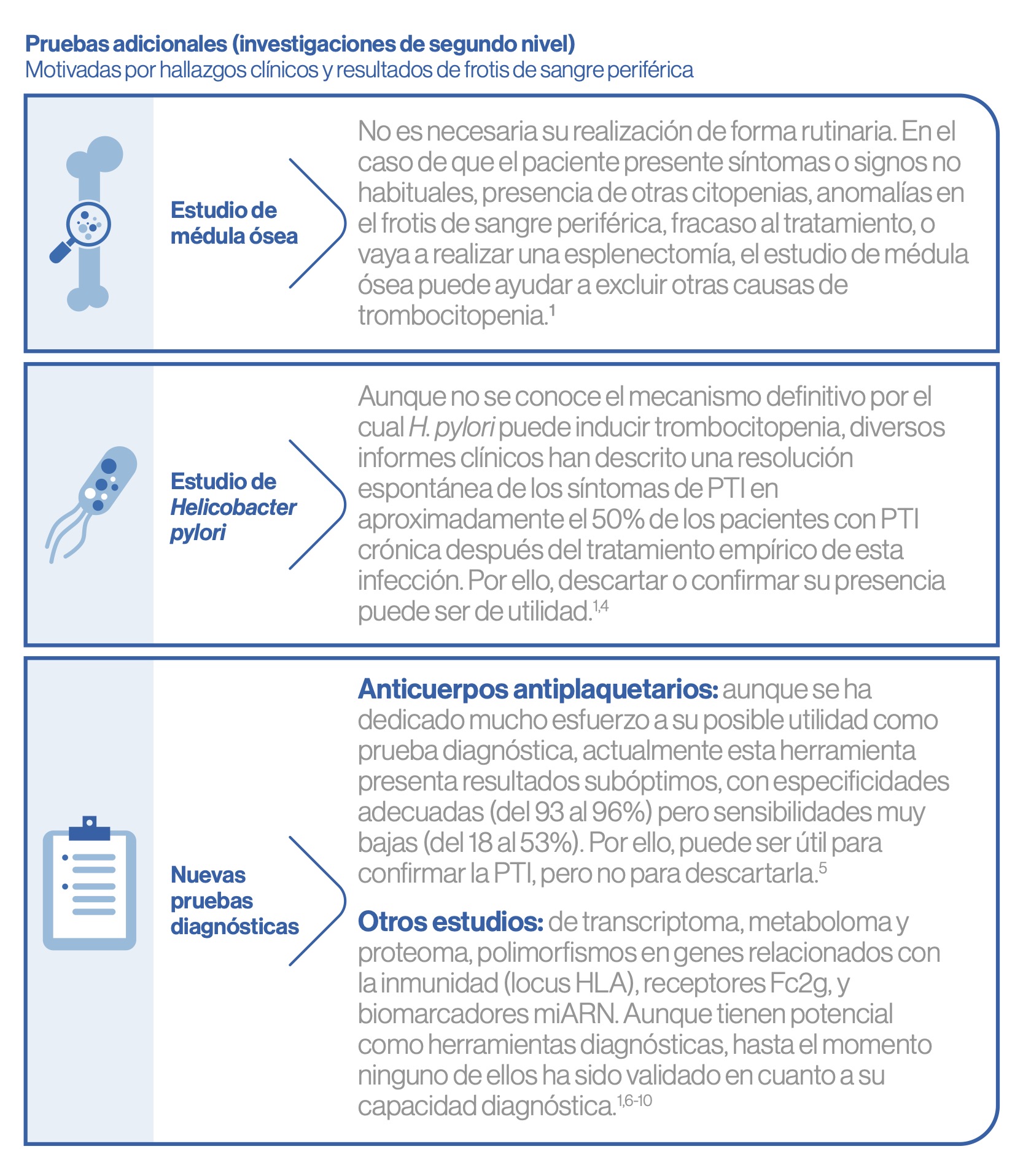
En la PTI – a diferencia de otras enfermedades – la ayuda de sofisticadas pruebas diagnósticas no suele tener gran valor. Esto puede suponer un gran desafío, ya que el diagnóstico diferencial de trombocitopenia es extenso.1
Aproximadamente un 20% de trombocitopenias inmunes se asocia a otros procesos subyacentes, lo que obliga a tener en cuenta otras causas de trombocitopenia, tanto inmunes (por ejemplo, secundarias a otras causas tales como infecciones, trastornos autoinmunes, o inmunodeficiencia), como no inmunes (inducidas por fármacos, por enfermedad hepática, por enfermedades de la médula ósea…).3
El diagnóstico preciso de la PTI sigue siendo difícil, y la prueba diagnóstica ideal para llevarlo a cabo de manera más rigurosa aún no se ha desarrollado. No existe una fórmula que permita un diagnóstico universalmente preciso y ninguna prueba se considera como altamente específica y sensible, consecuencia de que la enfermedad es la expresión clínica de una variedad de trastornos que, a través de diferentes mecanismos subyacentes, ocasionan trombocitopenia.1
Referencias:
1. Grupo de Trabajo de la SEHH y GEPTI. Directrices de diagnóstico, tratamiento y seguimiento de la PTI. 2021. Disponible en: https://www.gepti.es/images/stories/recursos/2022/02/GUIA-PTI-2021.pdf
2. Rodeghiero F, Stasi R, Gernsheimer T, et al. Standardization
of terminology, definitions and outcome criteria in immune thrombocytopenic purpura of adults and children: report from an international working group. Blood. 2009;113(11):2386-93
3. Moulis G, et al. Newly diagnosed immune thrombocytopenia adults: clinical epidemiology, exposure to treatments, and evolution. Results of the CARMEN multicenter prospective cohort. Am J Hematol. 2017;92(6):493-500.
4. Frydman GH, et al. Helicobacter pylori Eradication in Patients with Immune Thrombocytopenic Purpura: a Review and the Role of Biogeography. Helicobacter. 2015;20(4):239-51.
5. Vrbensky JR, Moore JE, Arnold DM, et al. The sensitivity and specificity of platelet autoantibody testing in immune thrombocytopenia: a systematic review and meta-analysis of a diagnostic test. J Thromb Haemost. 2019;17(5):787-94
6. Bal G, Futschik ME, Hartl D, et al. Identification of novel biomarkers in chronic immune thrombocytopenia (ITP) by microarray-based serum protein profiling. Br J Haematol. 2016;172(4):602-15.
7. Li Y, Li Y, Lu W, Li H, Wang Y, Luo H, et al. Integrated Network Pharmacology and Metabolomics Analysis of the Therapeutic Effects of Zi Dian Fang on Immune Thrombocytopenic Purpura. Front Pharmacol. 2018;9:597.
8. Ye QD, Jiang H, Liao XL, et al. Identification and Validation of Gene Expression Pattern and Signature in Patients with Immune Thrombocytopenia. SLAS Discov. 2017;22(2):187-95.
9. Audia S, Mahevas M, Samson M, et al. Pathogenesis of immune thrombocytopenia. Autoimmun Rev. 2017;16(6):620-32.
10. De Los Reyes-García AM, Arroyo AB, Teruel-Montoya R, et al. MicroRNAs as potential regulators of platelet function and bleeding diatheses. Platelets. 2019;30(7):803-8

